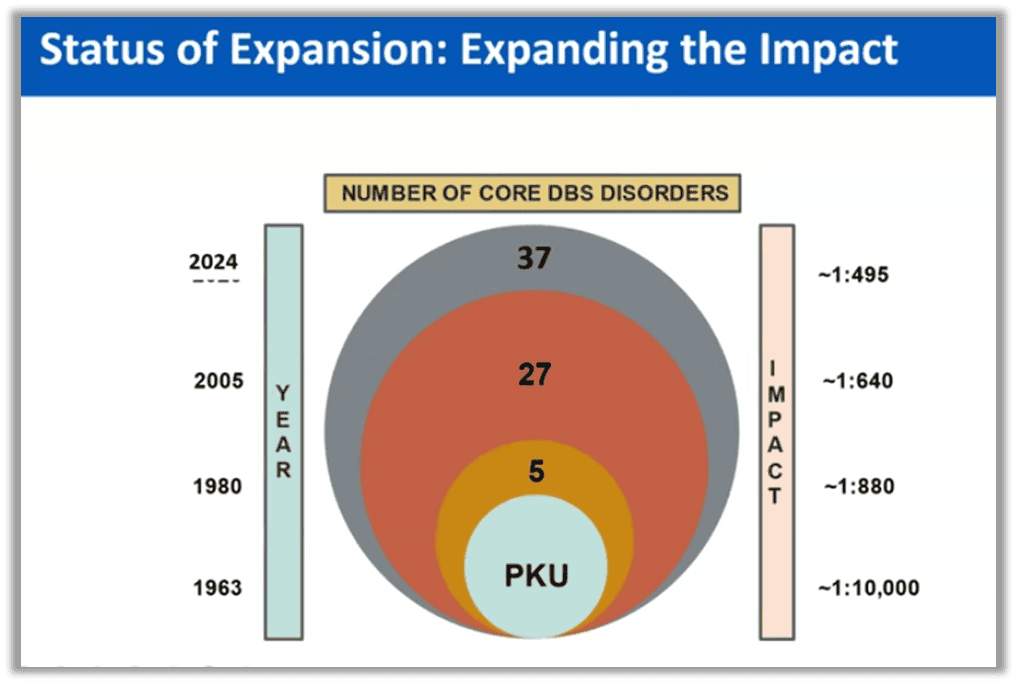
All newborns are required by state laws to have “newborn screenings” (NBS). In 1965 states started screening for one disorder, phenylketonuria (PKU) and at this point the federal government recommends screening for 39 “core” disorders or illnesses, and 26 secondary conditoins. Each state enacts their own policy, and state screenings range from 35 to 75 conditions.

Source: HRSA Data
Importantly, these screenings are done by “default,” as a “quasi-mandate,” and many parents have no idea their children are being screened for 35-75 diseases, nor what happens to the blood spot and data after it’s done. Parents can opt-out of the screening, or claim a religious exemption in the majority of states, but they can only do this if they know it’s happening – and CDC recommends screening happen right away, at 24-48 hours after birth.
It is well known and accepted that “Most NBS is done without parental consent.”
Source: Infants & Young Children
Keeping parents in the dark about screening isn’t just an oversight. It’s by design and promoted by organizations like the Association of Public Health Laboratories (APHL)…which reminds us the public health system sees parents as a barrier, not a partner.
Source: Parental Consent Out for Vote.pub
The APHL also takes the position that newborn blood spots should be able to be stored and used later without parental consent.
There are approximately 4 million babies born in the U.S. each year. What is the scope of the problem NBS is there for? “Annually, more than 6,500 infants are diagnosed with a disorder as a result of NBS.” The 37 core conditions chosen by the federal government as “core” to screen for are all conditions that could possibly cause serious health problems, disability, or death without medical treatment.
Newborn screening is described as a “quasi-mandate,” where parents are not asked and it will happen by default, but they can opt-out if they know to do so.
NBS is a “risk assessment” and prediction, not a diagnosis. But what happens if a family gets a medical prediction and they choose not to accept the recommended intervention? That remains to be seen, but we can make a good guess based on things like when parents refuse Vitamin K at birth, or refuse chemotherapy – in those situations, parents can lose custody of their child and the ability to have a say in their care. Right now, “Newborn screening does not have legislation specifying family rights and privileges, and there is no due process or dispute resolution procedure for families who are not satisfied with NBS services.”
Source: Newborn Screening: System Frameworks and Quality Assurance
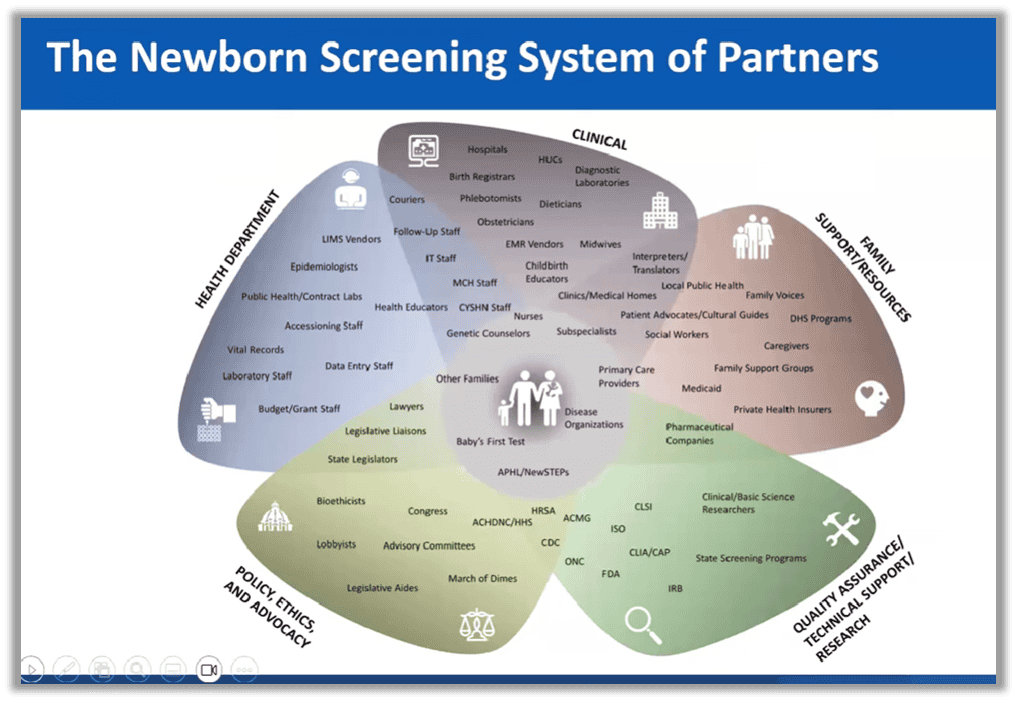
“Baby’s first test” is at the center of a whole lot of policy, clinical research, and more.
In the past, newborn screening expansion was limited by whether the technology existed. But that is rapidly changing. As technology evolves exponentially, the new limit is treatment.
Source: Bing Videos
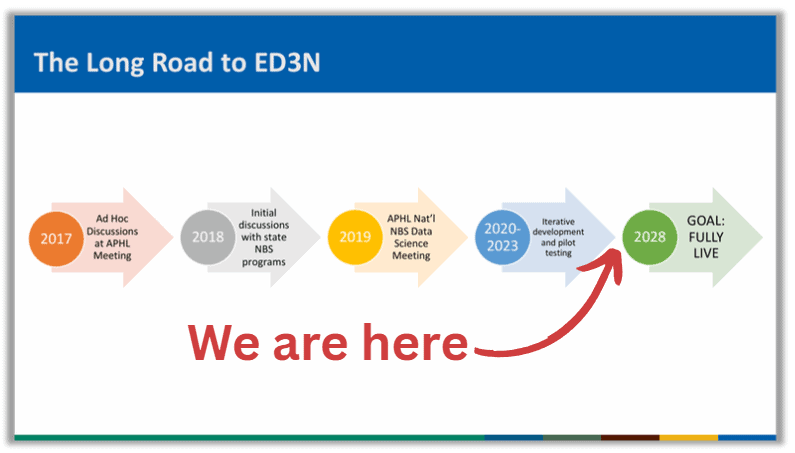
ED3N
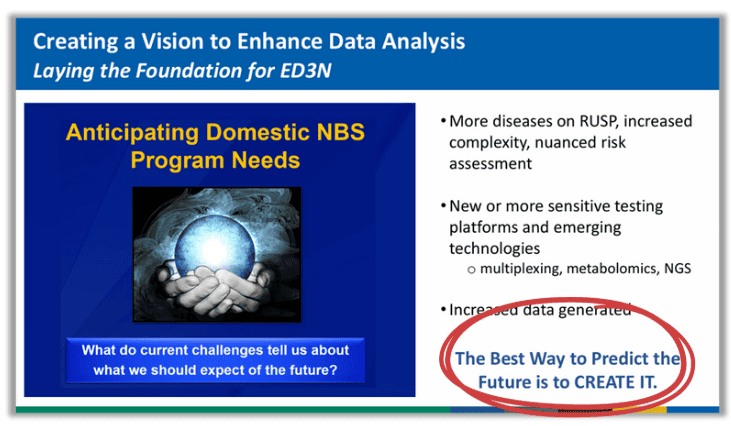
The federal government wants states to change their own policy to include DNA sequencing of babies at the same time they do the Newborn Screening already in place. The DNA is there, but the technology isn’t (yet). The CDC says the problem is, surveillance systems “are experiencing increased data analytic challenges associated with continued expansion of the number of newborn screening diseases, increased complexity of disease detection, and difficulties in correlating disease markers with disease risk.” The goal is to use artificial intelligence to do the screening. The CDC’s solution is a “new national newborn screening (NBS) data platform to serve as a secure, central, and national data sharing resource for the U.S. state and territorial NBS community.”
The CDC’s goal is to get data directly from laboratories with “near real-time patient data processing.” The creators acknowledge this will be a “mandated program,” and are exploring new technologies that could potentially protect patient privacy – a serious concern if an entire genome is being sequenced because how can data be deidentified if there is only one person on the planet with the data you’ve got in front of you?
One of the creators of ED3N explained the data would be “integrated at the patient level. This is going to be the beauty of ED3N is that we can actually look at the things from a patient perspective. We’re not going to be just looking at a biochemical data separate from the regular data, separate from clinical data, but will collect all pieces…” A statement like this makes one wonder how the CDC can claim DNA data can be de-identified and anonymous.
It’s also important to note that those involved with ED3N are “already working with the Department of Education in trying to figure out how [early intervention] and newborn screening can be linked.”
In promoting the data grab, the CDC says, “The best way to predict the future is to create it.” What do you think they plan to create in ED3N with our babies’ DNA?
Source: Wayback Machine
The ultimate goal for technocrats is to integrate Whole Genome Sequencing into all of medicine from womb to tomb.
The future of medicine is “personalized.” The New York Times reported on “The Ethical Minefield of Testing Infants for Incurable Diseases” in 2025, and warned: “Scientifically speaking, the possibilities are almost endless. Since virtually every disease has some basis in our genes, the full genome – with three billion base pairs, coding some 20,000 genes – contains a wealth of data to be mined for lifesaving intel and gut-wrenching secrets.”
Remember when people started removing their breasts because they believed they had a possibility (not certainty) of developing cancer down the line? This is the type of information we would be privy to with WGS. Right now NBS only screens for disorders we can treat. That’s out the window when we sequence the whole genome.
This raises a huge amount of ethical and legal concerns:
- One data breach is catastrophic because DNA is unchangeable. The implications range anywhere from privacy and medical disruptions to targeted biological warfare.
- How will the government be stopped from linking the DNA information to other databases, including those that have nothing to do with health? Will the DNA database ever be integrated into a digital identification?
- Do we want to live in a world where our lives are medicalized from the moment of birth until our deaths?
- How will parental rights and children be protected when a parent refuses predicted medical advice?
- How will a child be protected from discrimination and marginalization if there is something found in their DNA deemed unfavorable?
- Would this technology ever be moved from post-natal testing to pre-natal?
There is a way to go before WGS is tied to newborn screening, but that future is quietly closing in on us. Right now, the national infrastructure exists for newborn screening, and the missing link to WGS is for each state to invest in “Next Generation Sequencing” technology. That is the stepping stone to total surveillance in ED3N.
That is why this needs your attention now, before states build this out and hand our baby’s DNA to the federal government. Here are ways you can take action:
- Tell the CDC what you think about federal collection of baby DNA at this link.
- Find out where your state is in this process.
- Each state needs a data use agreement in order to feed data to the centralized ED3N system. You can call your state’s public health agency to find out if your state has one.
- You can research whether your state’s public health laboratory has begun investing in Next Generation Sequencing.
- Talk about this with everyone you can find, especially policymakers. Most people have no idea this is happening. Sunshine is the best disinfectant – sometimes policies are so horrible that they can only survive if no one knows about them…like a centralized database of all baby DNA collected without parental consent and held by the federal government.