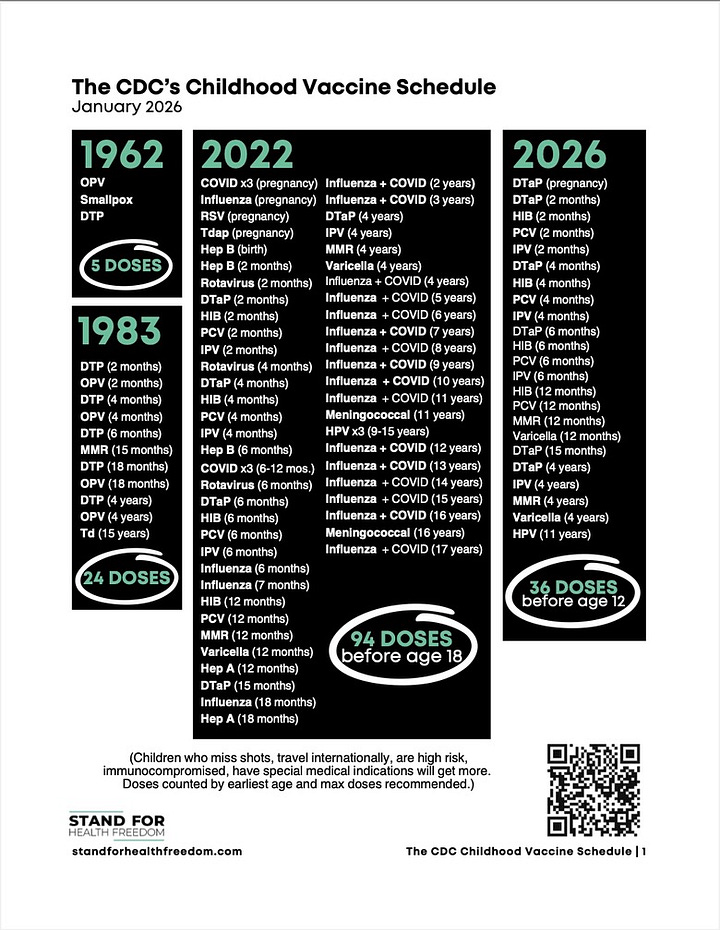
2026 started with a bang when the acting director of the Centers for Disease Control and Prevention (CDC), Deputy Secretary of Health and Human Services Jim O’Neill, announced historic changes to the CDC’s Recommended Childhood Vaccine Schedule on January 5th. When Mr. O’Neill’s boss, President Donald Trump took office one year ago, the CDC’s recommended childhood schedule looked like this:
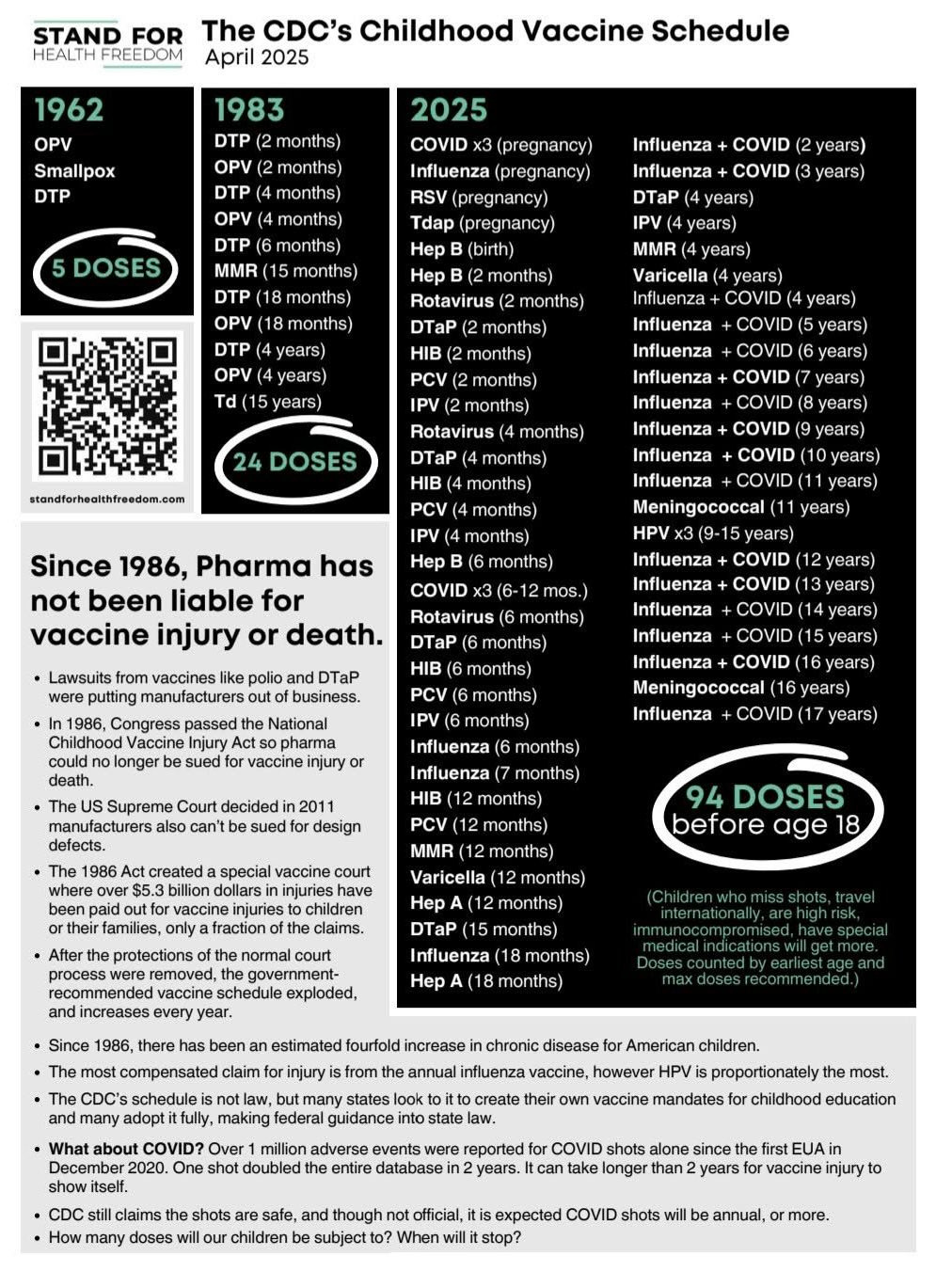
This behemoth of a schedule has only grown since the passage of the 1986 National Childhood Vaccine Injury Act, a law which effectively shields vaccine manufacturers and physicians from liability for vaccine-associated injury and death. The siren song of liability immunity is irresistible to vaccine manufacturers, as evidenced by the dramatic rise from 24 doses of 7 different vaccines in 1983 to the incredible high of 94 doses of 17 different vaccines, including annual covid vaccine boosters and RSV monoclonal antibodies, referred to as “immunizing agents,” in early 2025.
There was no end in sight.
Expectations were high, but changes to the childhood schedule were slow to take shape after the inauguration of President Trump and the confirmation of Robert F. Kennedy Jr. as Secretary of Health and Human Services. Immediate modifications to the CDC’s childhood schedule were unlikely in early 2025, given that Kennedy’s contentious confirmation hearings coincided with measles outbreaks in several states, along with the tragic deaths of two young girls, deaths the girls’ families attribute to medical neglect, though the media attributes them to measles.
Then, in May 2025, Secretary Kennedy took strategic action, completely bypassed the CDC’s Advisory Committee on Immunization Practices (ACIP), and removed the CDC’s general recommendation for COVID-19 vaccination for healthy children and pregnant women. Shifting the category to shared clinical decision making, a term meaning the universal recommendation for ALL patients is removed, and the patient now makes the final decision while considering information provided by their physician, like risks and benefits, as they should with every medical consideration.
It’s called voluntary informed consent.
Momentum shifted significantly when Secretary Kennedy removed all 17 ACIP members in June 2025, citing conflicts of interest. HHS also published a websitewhere conflicts of interest of ACIP members can be explored. Kennedy initially replaced them with eight new members: Dr. Martin Kulldorff (Chair), Dr. Joseph Hibbeln, Dr. Retsef Levi, Dr. Robert Malone, Dr. Cody Meissner, Dr. James Pagano, and Dr. Vicky Pebsworth. He has continued to add members over time, including five appointments in September – Dr. Catherine M. Stein, Dr. Evelyn Griffin, Dr. Hilary Blackburn, Dr. Kirk Milhoan, and Dr. Raymond Pollak – with two additional appointments as recently as January 13, 2026.
Changes and considerations to the CDC schedule made by the newly seated ACIP members in 2025 include:
- June 2025
- ACIP voted in favor of recommending clesrovimab (a long-acting RSV monoclonal antibody) for infants younger than 8 months.
- The committee voted to recommend annual influenza vaccination for individuals aged 6 months and older.
- The committee was presented information on thimerosal containing vaccines, delivered by L. Redwood, RN, MSN.
- ACIP voted against the use of thimerosal-containing influenza vaccines in key populations including children, pregnant women, and adults.
- September 2025
- ACIP formally recommended that COVID-19 vaccination be guided by individual-based decision-making (shared clinical decision-making) for people ages 6 months and older instead of a universal recommendation for 6 months plus and older.
- The committee voted to remove the recommendation of the MMRV vaccine from the recommended schedule.
- December 2025
- Regarding hepatitis b vaccination for infants born to women who test negative for hepatitis b, ACIP voted to recommend individual-based decision-making for parents deciding whether or not to administer a hepatitis B vaccine, including the birth dose. This essentially moved hepatitis b vaccination off the recommended childhood schedule. ACIP suggested in its recommendation that for parents who do decide to give the hepatitis b vaccine, the initial dose be administered no earlier than two months of age. (This is not a recommendation for a hep B series beginning at two months, rather a suggestion that if you do vaccinate your infant, don’t do it before age 2 months.)
- The committee voted to recommend that parents evaluate the need for a follow-up dose and suggested they conduct a serology test prior to a second dose. This was a huge admission that individuals react differently to vaccination and should be treated based on individual physiology, not a recommended, one-size-fits-all schedule.
Two extraordinary presentations were made during the December ACIP meeting:
- Attorney Aaron Siri presented a history of the childhood/adolescent immunization schedule including the evolution of the childhood/adolescent vaccination schedule in the U.S., and a vaccine schedule comparison: U.S. and other developed countries.
- Dr. Tracy Beth Hoeg of the FDA presented a comparison of the U.S. vs. Danish vaccine schedule.
The momentum for a reduced vaccine schedule grew slowly, but the December ACIP meeting was a tipping point. As the meeting ended on December 5th, President Trump posted to social media:
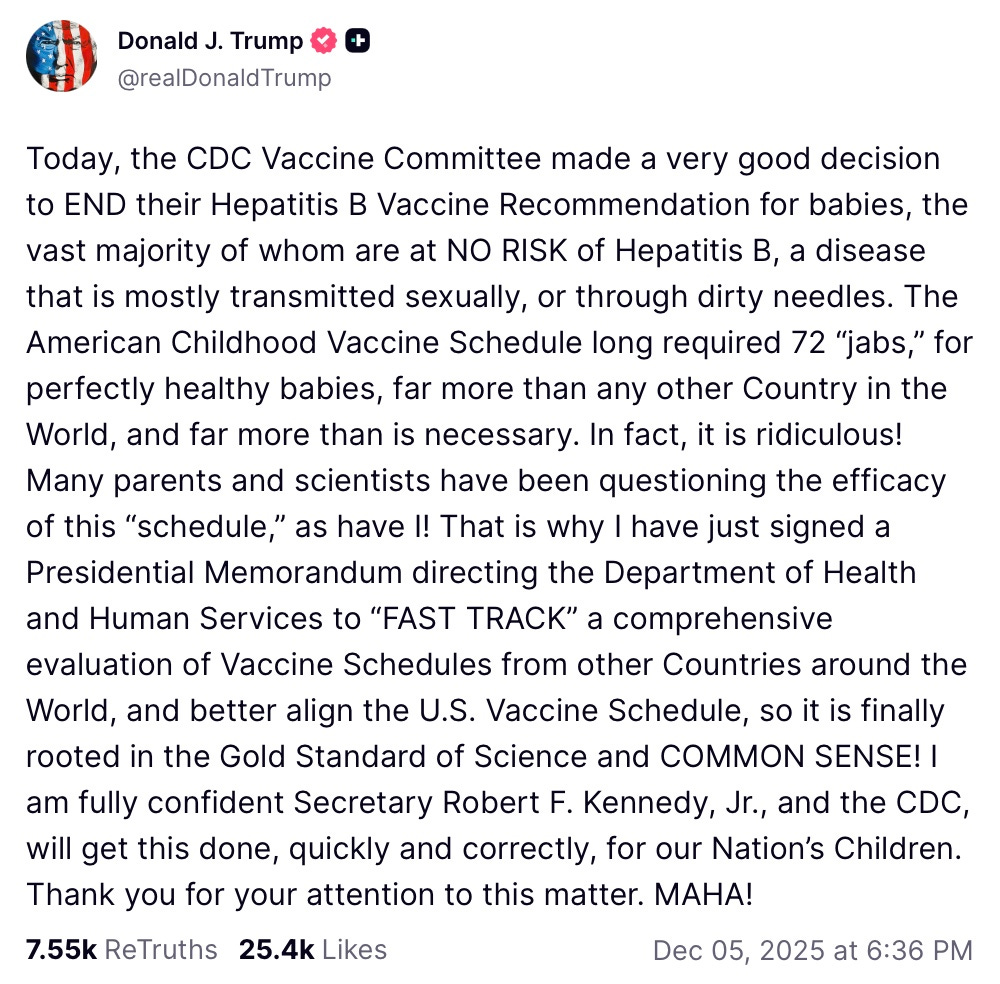
Matching words with action, Trump immediately issued an official directive for the U.S. shot schedule to be evaluated in comparison to other countries.
“I hereby direct the Secretary of Health and Human Services and the Director of the Centers for Disease Control and Prevention to review best practices from peer, developed countries for core childhood vaccination recommendations — vaccines recommended for all children — and the scientific evidence that informs those best practices, and, if they determine that those best practices are superior to current domestic recommendations, update the United States core childhood vaccine schedule to align with such scientific evidence and best practices from peer, developed countries while preserving access to vaccines currently available to Americans.”
Exactly one month later, on January 5, 2026, CDC Acting Director Jim O’Neill announced that the agency would adopt recommendations put forward by Dr. Jay Bhattacharya, Director of the National Institutes of Health (NIH); Dr. Mehmet Oz, Administrator of the Centers for Medicare and Medicaid Services (CMS); and Dr. Marty Makary, Commissioner of Food and Drugs (FDA). Under these recommendations, the childhood immunization schedule would be substantially revised to more closely align with those of other developed countries. They write:
“The scientific assessment compared U.S. childhood immunization recommendations with those of peer nations, analyzed vaccine uptake and public trust, evaluated clinical and epidemiological evidence and knowledge gaps, examined vaccine mandates, and identified next steps.”
The new guidance divides vaccination recommendations into three groups: Immunizations Recommended for All Children, Immunizations Recommended for Certain High-Risk Groups or Populations, and Immunizations Based on Shared Clinical Decision Making.
The immunizations recommended for all children has been pared down to those deemed “consensus vaccines,” and include: measles, mumps, rubella, diphtheria, tetanus, pertussis, polio, Haemophilus influenzae type B (Hib), pneumococcal disease, human papillomavirus (HPV), and varicella. This reflects the Danish schedule with the exception of the varicella vaccine – more on that in a moment.
Seven vaccines moved to the newly created “shared clinical decision making” schedule and include: hep B (as of the last ACIP meeting), COVID-19 (as of last year), hep A, rotavirus, meningococcal, influenza, and respiratory syncytial virus (RSV) monoclonal antibodies.
High risk groups are now recommended RSV, hepatitis A, hepatitis B, meningococcal B, meningococcal ACWY, and dengue vaccines.
No changes were made in regards to coverage “without cost sharing by private insurance and covered by Medicaid, Children’s Health Insurance Program (CHIP), and the Vaccines for Children Program.”
The announcement concedes serious concerns previously dismissed, as well as a shocking admission about the serious implications of interrupting natural immunity with widespread use of a vaccine. In a particularly compelling admission, the CDC announcement acknowledges that the varicella (chickenpox) vaccine will remain a consensus vaccine even though other peer nations do not recommend it because “stopping use of this vaccine could cause certain complications.” Specifically, once widespread use of varicella is adopted, discontinuing its use “could increase the average age at which the population naturally gets chickenpox when this disease could cause more complications.”
Below are direct quotes from the CDC document:
- The Institute of Medicine (IOM) stated in a report that “vaccines—like all drugs or medical interventions—are neither 100 percent risk-free nor 100 percent effective.”
- The United States administers significantly more doses of childhood immunizations than its peer nations, yet there is a significant knowledge gap due to a dearth of randomized vaccine trials and limited post-licensure infrastructure for monitoring potential adverse reactions and long-term chronic events.”
- The U.S. has a limited post-licensure infrastructure focused on monitoring potential adverse reactions that occur within a few days or weeks after vaccination.
- Additionally, current surveillance systems are underutilized to detect long-term harms.
- The mere existence of a vaccine does not automatically make it appropriate for every child, nor does it necessarily justify universal vaccination.
- There is global variation in the universal use and timing of numerous childhood vaccines. Although these differences sometimes reflect the unique epidemiology of diseases in each region, they more often arise from uncertain science and knowledge gaps, which lead to inadequately informed assessments of risks and benefits that are subject to differing interpretations.
- Shared clinical decision-making recommendations are individually based and informed by a discussion between the health care provider and the patient or parent/guardian, something that should occur for all vaccines.
- Sometimes, it is also important to consider personal and family preferences, beliefs, and knowledge, including when a patient presents specific information regarding the pre-and-post licensure safety data of a vaccine or presents specific familial experience with a vaccine.
These are shocking admissions we never thought would be made from a federal health agency, but perhaps the most significant was saved for last. The final paragraph of recommendations from NIH, CMS, and FDA addresses one of the major concerns in Stand for Health Freedom’s lawsuit against the CDC:
“Finally, if you approve the revised schedule, you should also later recommend to the Secretary that HHS agencies fund and conduct gold standard medical research to assess overall health outcomes related to all immunizations on the revised schedule (i.e., immunizations recommended for all children, immunizations recommended for high-risk groups, and immunizations based on shared clinical decision making), the interaction effects between different immunizations as well as other aspects of the immunization schedule – something that is needed to close the knowledge gap.”
These are damning concessions, reaffirming the necessity of SHF’s lawsuit against the CDC and validating our nationwide effort to remove mandates in all 50 states with the passage of the Medical Freedom Act.
The revised childhood schedule reflects a dramatic reduction in the number of recommended shots, especially striking when contrasted with the extraordinarily high number of injections children faced at the beginning of 2025.
Absent intentional intervention, the number of shots recommended for all children would have continued to rise, not fall.
Stand for Health Freedom’s updated shot schedule flyer truly reflects how far we’ve come, and how far we have yet to go to ensure every one of these shots is properly assessed for safety and free of coercion.
Some states, encouraged by professional organizations like the American Academy of Pediatrics (AAP), are sticking to the January 2025 CDC schedule. For the first time in modern public health history, there is no single, unified government and industry opinion guiding childhood vaccination in the United States. Even the CDC announcement notes:
“Disagreement among states and professional societies in the U.S. further underscores the need and opportunity for a more adaptable childhood immunization schedule.”
Vaccine choice and informed consent are center stage in national conversation. When giants disagree, it shows us the illusion of “settled science.” You can see the cracks – professional organizations, states, the federal government, policymakers and scientists alike are fighting it out on the national (even international) stage.
And this absence of consensus reminds us of the significance of the mother’s role. As a mother, your intuition, your education, your values, and your informed consent matter now more than ever. Do you want the real info?
We are proud to offer this resource to you: The Vaccine Decision, Every Shot Has a Story.
No matter what your state has chosen to mandate, this book remains a tool to help you understand the history, assumptions, risks, and decision-making frameworks surrounding the vaccine schedule, so you can discern where you stand, free from fear and pressure.
Our prayer is that you move forward confidently in your God-given authority to protect, nurture, and care for your child.