April 17, 2024 – We are less than five weeks away from the 77th World Health Assembly, where votes are scheduled on the pandemic treaty and the amendments to the International Health Regulations (IHR).
For the very first time, on April 17, 2024, almost three months after the deadline, we have seen the first draft of proposed amendments to the IHR (2005). Additionally, we have a new leaked version of the pandemic treaty that looks drastically different from previous drafts. Notably, both failed to be submitted in time, per the International Health Regulations, and neither should be up for a vote in May. But the World Health Organization is plowing ahead, having declared its own rules do not apply to them. The legality of the vote will surely be challenged assuming they move forward.
Clearly, there’s an urgency to get something, anything in place, even if the documents look like Swiss cheese.
In short, both of the documents have been seriously scaled back in content, but not in scope. We used to hear the phrase, “Nothing is agreed until everything is agreed,” but at this point it looks like all we’re aiming for is to agree to anything and fill in the details later.
“You can’t chicken out now” -Precious Matsoso, Co-Chair, opening remarks, pandemic treaty meeting #9.[i]
“There are very real risks if we do not reach an agreement in May.” –Pamela Hamamoto, U.S. delegate in charge of pandemic treaty negotiations, at pandemic treaty meeting #9 (emphasis added).[ii]
IHR amendments update:
The proposed bureau’s text of the IHR amendments is much more sparse than one would anticipate based on the submission of over 300 amendments and the culmination of 14 months of work to compile them.[iii] But the changes are still significant.
- A new “pandemic emergency” term is defined, which essentially broadens the scope of the IHR to pandemics that haven’t happened but are deemed “likely.” Is the potential pathogen “likely to” spread, overwhelm health systems, cause “social and/or economic and/or political disruption,” and require rapid response? This is the veiled increase of the “PHEIC” from one single declaration to the ability to declare an emergency for a “likely” threat.
- A new IHR Compliance Committee would be created, “with a view to assisting States Parties to comply with their obligations and strengthen core capacities.” It is not spelled out how that will happen, nor have any limits have been placed on the committee.
- There are increased financial contributions, commitments, and promises called for throughout the document, especially to “assist” developing countries. Shockingly, China claims the status of a developing country. Equitable access to “health products” is a featured amendment throughout the document, meaning poor (“developing”) countries want more resources from rich countries – and they want that promise in writing.
- We already have a “National Focal Point” to communicate directly with the WHO about IHR implementation in our country. Amendments would add another office for the National IHR Authority, which would be responsible for making sure the IHR is implemented in the country.
- A new definition for a “product dossier” is added for health products submitted for marketing authorization on the global stage for “prequalification or emergency use listing.” This sounds eerily like a global Emergency Use Authorization.
- And while WHO Director-General Tedros Adhanom Ghebreyesus continues to say the WHO will not take over state sovereignty through these documents, we do see this new language:
“WHO shall collaborate with, and assist, States Parties, upon request, to the extent possible in…strengthening domestic legislative and administrative arrangements for the implementation of these Regulations.” (Bolded language is new).
Being a part of this agreement means changing U.S. law to be in line with WHO decisions, and there will be a new Compliance Committee to “facilitate and oversee” that process.
The Working Group for the International Health Regulations (WGIHR) is meeting this week, April 22-26, with the intent of buttoning up this draft so the entire international focus can be on making sure the treaty draft will pass at WHA 77.
Treaty update:
The last pandemic treaty draft was released March 13, and another leaked around April 17, 2024. The latest draft is remarkably lighter than previous attempts. Some are referring to the new treaty draft as a “placeholder” document, where basically countries would agree to be bound to something even though the details aren’t worked out yet. It’s a blind agreement. The next, and presumably final, meeting of the Intergovernmental Negotiating Body (INB) that is working on the treaty, spans April 29 – May 10.
The latest leaked “Proposal for the WHO Pandemic Agreement,” is very different from previous drafts. Many of the contested details have been removed, and instead there are promises that the blanks will be filled in after the treaty is adopted.
Here is a sampling of blank checks found in this leaked document:
- Article 5.4: We want people = animals = environment, but we’ll tell you what that means later and coordinate it with a treaty that looks one way right now, but will look very different later.
“The modalities, terms and conditions, and operational dimensions of a One Health approach shall be further defined in an instrument, that takes into consideration the provisions of the IHR (2005), [to which over 300 amendments have been proposed and are not finalized] and is operational by 31 May 2026.”
- Article 6.5: We’re going to check in regularly on how well you’re following our new rules under the watchful eye of a new around-the-clock global health governing body, once they form and set up their rules.
“With the aim of promoting and supporting learning among Parties, best practices, and accountability and coordination of resources, an inclusive, transparent, effective and efficient pandemic prevention, preparedness and response monitoring and evaluation system shall be developed, implemented and regularly assessed, by WHO in partnership with relevant organization, building on relevant tools, on a timeline to be agreed by the Conference of the Parties.”
- Article 12.6: We want everyone to share pathogens with each other, as well as the monetary or other gains from them, but we know we can’t get everyone on the same page with this. So rather than sink the treaty ship, we’ll promise to figure it out after we agree on doing it regardless of what it looks like.
“The modalities, terms and conditions, and operational dimensions of the PABS [Pathogen Access and Benefit-Sharing] System shall be further defined in a legally-binding instrument, that is operational no later than 31 may 2026.
- Article 13.2: We’re going to let the new global health governance body take over on deciding who has access to pandemic products through our new Global Supply Chain and Logistics Network.
“The Conference of the Parties shall, at its first meeting, define the structure and modalities of the [newly created Global Supply Chain and Logistics] Network…”
- Article 13.6: We want to remove liability from manufacturers and distributors of vaccines and pandemic products at a global level, but we won’t put it in the treaty directly; it can be amended later.
“A multilateral system for managing vaccine and therapeutic related compensation and liability during pandemics shall be considered.”
- Article 20.4: In addition to the Pandemic Fund at the World Bank, we want more “sustainable and predictable financing” especially for surge funds to poor countries. The new global health governance body will seek out promises for more funding from countries and organizations, and we’ll let them determine how to set that up.
“The Conference of the Parties shall adopt terms of reference for the [Coordinating Financial] Mechanism and modalities for its operation and governance, within 12 months after the entry into force of the WHO Pandemic Agreement.”
- Article 21: We’re establishing a global health governance body completely separate from the World Health Assembly that can be in force all the time, and will decide on how it will govern itself, and how it will make sure countries are complying with the treaty. It can create additional subordinate bodies and dictate finances at will.
“[I]t shall take actions, as appropriate, for the achievement of the objective of the WHO Pandemic Agreement…[it] shall by consensus adopt financial rules for itself…[and] may establish subsidiary bodies, as it deems necessary, and determine the terms and modalities of such bodies.”
- Article 31: That independent global health governing body will be able to change the pandemic treaty and they will decide on the procedure for doing so and how fast it can happen.
“The Conference of the Parties may adopt protocols to the WHO Pandemic Agreement….The requirements for entry into force of any protocol, and the procedure for the amendment of any protocol, shall be established by that instrument.”
It’s also notable that the treaty proposes a lower threshold for adopting amendments to the treaty than the IHR already has in place. It puts into writing that States “shall make every effort to adopt any proposed amendment to the WHO Pandemic Agreement by consensus,” not by WHA vote. But in the case they must vote, oddly a three-quarters majority is required, which is more than the two-thirds required to pass the treaty to begin with. The amendments would go into force in 90 days, rather than the one-year process (shortened by 2022 amendments from two years) in the IHR. No mention is made that treaty amendments must be ratified by the countries. This can be read as: Once we pass this treaty and your country ratifies it, there’s no more input, so they can fill in all those blank checks at will.
But wait, there’s more! U.S. Global Health Security Strategy update:
In addition to the treaty and the IHR Amendments, the U.S. is hedging its bets by moving ahead with updates to its own Global Health Security Strategy, which looks very similar to the proposals on the global stage. This, however, is domestic policy that the U.S. does not have to run through the World Health Organization to implement.
This document on its own is evidence we do not need a global health governance, nor a seat at the World Health Organization’s table, in order to influence global health policy, help other nations in need, and affect global health security. (Click here to learn about the WHO Withdrawal act, and urge your lawmaker to sign on if they haven’t yet!)
Here’s one stand-out goal of the updated U.S. Government Global Health Security Strategy of April 2024:[iv]

Translation: Everything becomes public health. Health security will span multiple agencies across the federal government, including defense.
The One Health approach is significant because we have a government of enumerated powers. In other words, our government only has the power we give them. If an individual or an agency works outside of the scope they were assigned, it’s unconstitutional. One Health is the Midas Touch that turns everything into public health.
Here is how the CDC describes One Health[v]:

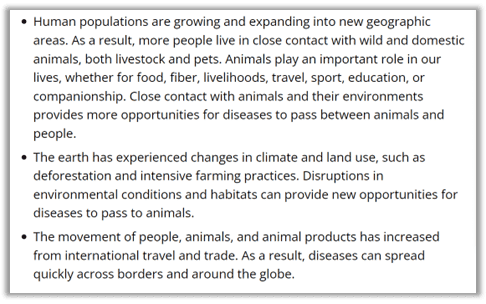
The CDC explains that human population growth, climate changes, land use, and travel cause disease. You can see how this quickly swallows up basically every human activity into a health activity.
As Stand for Health Freedom revealed in an analysis of early-filed state bills in the 2024 session, the WHO claims jurisdiction over a wide variety of things. We found over 300 bills that pointed to the WHO as an expert in fields you may not expect:
You can easily print and share our PDF “The invisible hand of the WHO in the states,” with friends and lawmakers, so they can get a visual grasp on what WHO does at the state level.
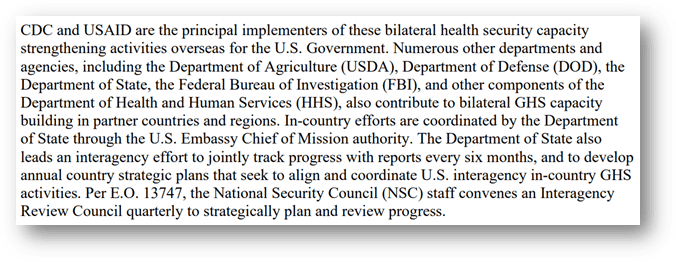
Here’s another excerpt showing the health policy mission creeping across the government:
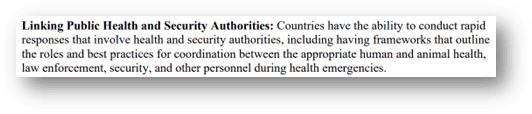
And in case you still have any doubt about the security part of the global health security agenda, here’s one of the highlighted goals:
Conclusion:
This is where we stand: Two potentially illegal votes are scheduled for the end of May 2024 at the 77th World Health Assembly. The proposed changes to the IHR have been scaled back in detail, but not in scope, as the addition of “pandemic emergency” as a “likely” threat expands the ability for the WHO to make declarations and recommendations, provide guidance, and require funds. Between the two treaties, we’d potentially have another point of contact on the shores of the U.S. to ensure implementation of the IHR, in addition to two new global bodies that would “oversee” and in some way “facilitate” compliance with WHO decisions.
We don’t know what will happen at the WHA. We do know it is much harder to get the treaty passed than the IHR amendments. The treaty requires a two-thirds majority in the WHA and ratification by member states, in the U.S. that means two-thirds support of the Senate. The IHR requires only a simple majority vote in the WHA and no U.S. Senate involvement for it to become binding on the U.S. people.
We also know that regardless of the IHR or the treaty, the White House is bound and determined to move forward with a global health security strategy all its own.
Take Action
What do we do now? We wait; we watch; we vote. Keep informed about WHO happenings by checking our social media and getting our email list!
[i] “A/INB/9.” World Health Organization. March 28, 2024. Video, https://apps.who.int/gb/inb/e/e_inb-9.html., Agenda Item 1 & Agenda Item 2, part 1 video, around 6 minutes.
[ii] “A/INB/9.” World Health Organization. March 28, 2024. Video, 1:02:30, https://apps.who.int/gb/inb/e/e_inb-9.html.
[iii] “Working Group on Amendments to the International Health Regulations (2005) (WGIHR).” WHO. April 17, 2024. https://apps.who.int/gb/wgihr/pdf_files/wgihr8/WGIHR8_Proposed_Bureau_text-en.pdf.
[iv] “U.S. Government Global Health Security Strategy 2024.” White House. April 1, 2024. https://www.whitehouse.gov/wp-content/uploads/2024/04/Global-Health-Security-Strategy-2024-1.pdf.
[v]“One Health Basics.” CDC. September 28, 2023. https://www.cdc.gov/onehealth/basics/index.html#:~:text=One%20Health%20is%20a%20collaborative,plants%2C%20and%20their%20shared%20environment.